Why some countries are mixing-and-matching vaccine doses?
There are promising signs of improved immune response even against variants of concern, but the jury is still out.
KINIGUIDE | During a webinar on Tuesday, National Covid-19 Immunisation Programme (NIP) Coordinating Minister Khairy Jamaluddin said Malaysia is looking into offering the Pfizer-BioNTech vaccine for those who have received the AstraZeneca vaccine as their first dose.
Not only that, but he also said it is “possible” that Malaysia would adopt this strategy, which seems to have evoked mixed responses from netizens.
In this instalment of KiniGuide, we look into the heterologous prime-boost vaccination strategy and why this is being studied.
What is heterologous prime-boost?
Using the same vaccine multiple times to boost immunity is known as “homologous prime-boost” and is used in most vaccines, including those that protect against Covid-19.
However, the alternative strategy of using different vaccines for the first dose (priming dose) and subsequent doses (booster dose) has been studied for other diseases since at least 1992.
This is the heterologous prime-boost protocol, which seemed to elicit a more robust immune response but also drove up the cost and complexity of developing and deploying the vaccine. The strategy has found some early success in the vaccine for preventing Ebola.
For preventing Covid-19, the Sputnik V vaccine is designed as a heterologous prime-boost vaccine from the outset and has reported 91.6 percent efficacy in clinical trials.

The Sputnik V vaccine uses two different viruses - both rendered harmless - to deliver temporary genetic instructions into human cells for producing a protein found outside of the virus that causes Covid-19.
The body’s immune system then recognises these proteins as foreign objects and mounts the necessary immune response.
Packaging for the Sputnik V vaccine is colour-coded red or blue to help differentiate between the two doses.
With some exceptions such as the Sputnik V, however, most countries have not recommended heterologous prime boosting against Covid-19 due to a lack of data to support its use. Nevertheless, the situation is beginning to shift.
What did Khairy say about mixing vaccine doses?
During a webinar hosted by the Oxford & Cambridge Society of Malaysia on Wednesday (June 16), Khairy was asked a question from the audience on whether the government is considering offering the Pfizer-BioNTech vaccine as the second dose to people who have received the AstraZeneca vaccine as the first.
This is in light of the poor performance of the AstraZeneca vaccine in preventing mild-to-moderate disease caused by the Beta variant (B.1.351) of Covid-19, which is circulating in Malaysia.
In response, Khairy revealed that Institute of Clinical Research (ICR) director Dr P Kalairasu had last week presented a paper on the issue to the Special Committee for Ensuring Access to Covid-19 Vaccine Supply (JKJAV).
“We have some real-world data that we received from Germany about heterologous vaccinations using AstraZeneca for the first dose and Pfizer for the second dose, which has been shown to boost the neutralising antibodies and to be more effective against variants.
“We are watching this very closely. We don't want to make a quick decision on this before getting more data. The data points are coming in for heterologous vaccinations.
“Once the technical working group (led by Kalairasu) is clear on that, they'll advise the committee that I chair with the health minister, and we will implement heterologous vaccinations.
“It is possible that we will end up doing this because a lot of countries are doing this to boost the neutralising antibodies, to boost the efficacy or effectiveness, and also when you are facing vaccine supply constraints, you can mix things up and ensure the effectiveness of the vaccine is still there,” he said.
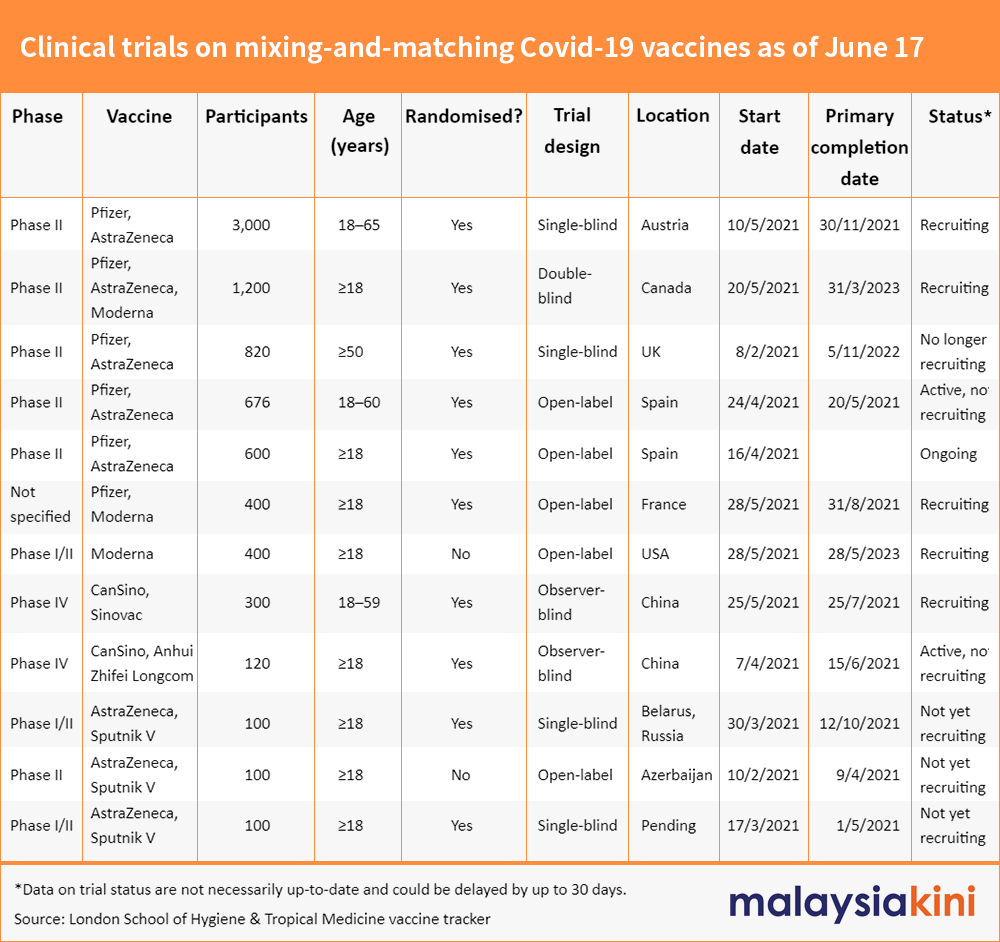
What are the studies looking at heterologous prime boosting?
According to data compiled by the London School of Hygiene & Tropical Medicine, there are at least 12 clinical trials studying mixing and matching various Covid-19 vaccines as of June 14.
They cover various combinations of vaccines from different pharmaceutical companies including Pfizer, AstraZeneca, Moderna, Cansino Biologics, Sinovac and Sputnik V.
Some of these studies investigate switching vaccines for the second dose, while others look at using a different vaccine to boost immunity for people who have already completed their vaccination months earlier.
The list excludes other types of studies, such as observational studies.
What do they have to show for?
Some preliminary results from these studies have begun to trickle in since May.
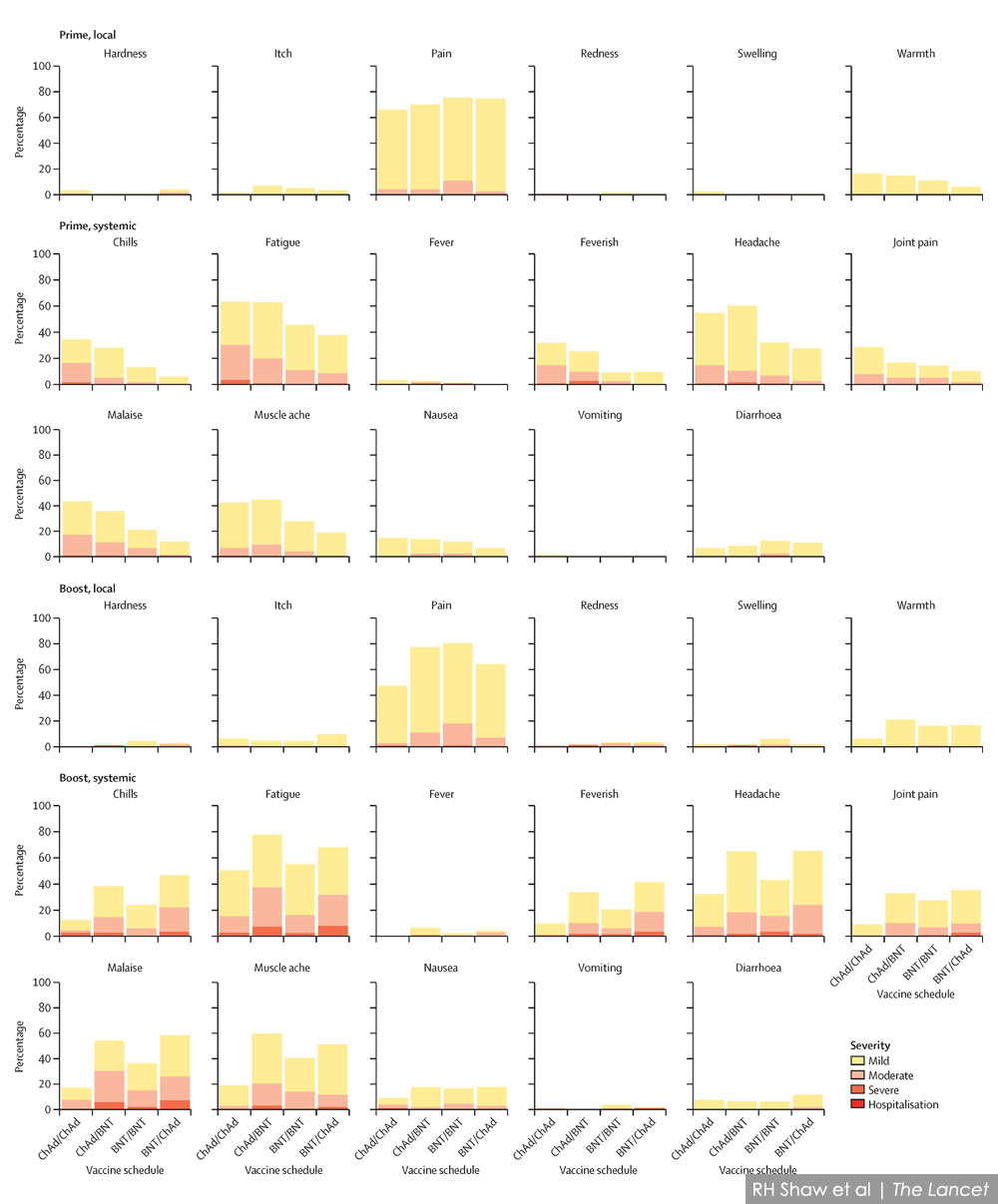
One study in the UK investigated four different combinations of the Pfizer-BioNTech vaccine and the AstraZeneca vaccine.
They reported when a different vaccine is given as the second dose, more people report a range of common vaccine side effects compared to those who received two of the same vaccine.
These side effects are generally of mild-to-moderate severity, such as fever, chills, fatigue, headaches and joint pain. None of the participants required hospitalisation.
According to a Reuters report on May 19, data on the immune response is expected in the coming months.
In the Spanish study, meanwhile, researchers recruited people who have already received one dose of the AstraZeneca vaccine; and randomly assigned them to either receive the Pfizer-BioNTech vaccine as the booster shot, or no booster at all.
They found that participants who received the Pfizer-BioNTech booster shot produced higher levels of antibodies capable of neutralising the virus that caused Covid-19, compared to levels expected if they had received the AstraZeneca vaccine as their second dose instead.
A study in Germany is the most promising so far, but has to be interpreted with extra caution because it is limited by its small size and by not having a comparison group.
Researchers recruited 26 people aged between 25 and 46 years who have received one dose of the AstraZeneca vaccine and gave all of them the Pfizer-BioNTech vaccine eight weeks after their first dose.
Unlike the UK study, they found participants generally experienced milder side effects after the second dose, compared to the first dose. The most serious was one or two cases of headache and fatigue that lasted more than a day.
In terms of antibody response, they found it to be 3.9 times more potent in neutralising the Alpha variant (B.1.1.7) than would have been expected from people receiving two doses of the Pfizer-BioNTech vaccine.
This potency was cut in half when tested against the Beta variant that is capable of evading antibodies elicited by the current crop of vaccines, but despite this, the high antibody levels meant it remained effective in neutralising the virus.
The German-based researchers also said they tested against the B.1.617 variant but did not specify whether it is the Delta subvariant (B.1.617.2) that is linked to outbreaks in the UK, India and Labuan, or the Kappa subvariant (B.1.617.1) that is considered a “variant of interest” rather than a “variant of concern”.
In this case, mixing vaccine doses was found to be as effective against B.1.617 as it was against the Alpha variant.
There is also another study based in Germany that involved 129 healthcare workers who were given the AstraZeneca vaccine as the first dose, and the choice of either the AstraZeneca vaccine or the Pfizer-BioNTech vaccine for their second.
It similarly found a stronger antibody response that is effective when tested against the original Covid-19 strain first detected in Wuhan, China, as well as the Alpha, Beta and Gamma (P.1) variants. It said the high levels are similar to those who received two doses of the Pfizer-BioNTech vaccine.
However, data from across these four studies still leave a key question unanswered: How effective is it in the real world?
While a higher antibody response generally means greater protection against Covid-19, antibodies are only one facet of a complex immune response.
It is still poorly understood how blood markers such as antibody levels and other immune cell responses can be used to predict a vaccine’s effectiveness in the real world.
These “correlates of protection” are still an active area of research, and so are the efficacy of various vaccine combinations. As mentioned earlier, more data are expected in the coming months.
It should also be noted all four studies detailed above are not peer-reviewed, but the papers have been made publicly available.
Why mix-and-match vaccines in the first place?
Based on earlier experiences in developing vaccines, the heterologous prime-boost protocol is already known to produce a greater immune response.
This has garnered greater importance following the appearance of Covid-19 variants that can evade some of the antibodies elicited by the current crop of vaccines, alongside other strategies such as offering a third vaccine dose or developing updated versions of the vaccines.
Heterologous prime boosting also addresses a limitation in viral vector vaccines that caused concern that it could lose potency if used repeatedly as booster shots, especially if Covid-19 becomes endemic and such boosters become necessary for years to come.
Viral vector vaccines (such as the Sputnik V vaccine and vaccines from AstraZeneca, Johnson & Johnson, and CanSino Biologics) work by repurposing a harmless virus as a messenger to deliver genetic instructions for producing a component of the other virus that causes Covid-19.
It is feared that with repeated doses, the body could develop immunity against the vector itself, essentially killing the messenger before the message could be delivered.
Using different vectors is seen as a way to bypass this limitation, but thus far, Financial Times quoted sources claiming that the AstraZeneca vaccine remains effective as a third dose booster and is “strong enough for any variant”.
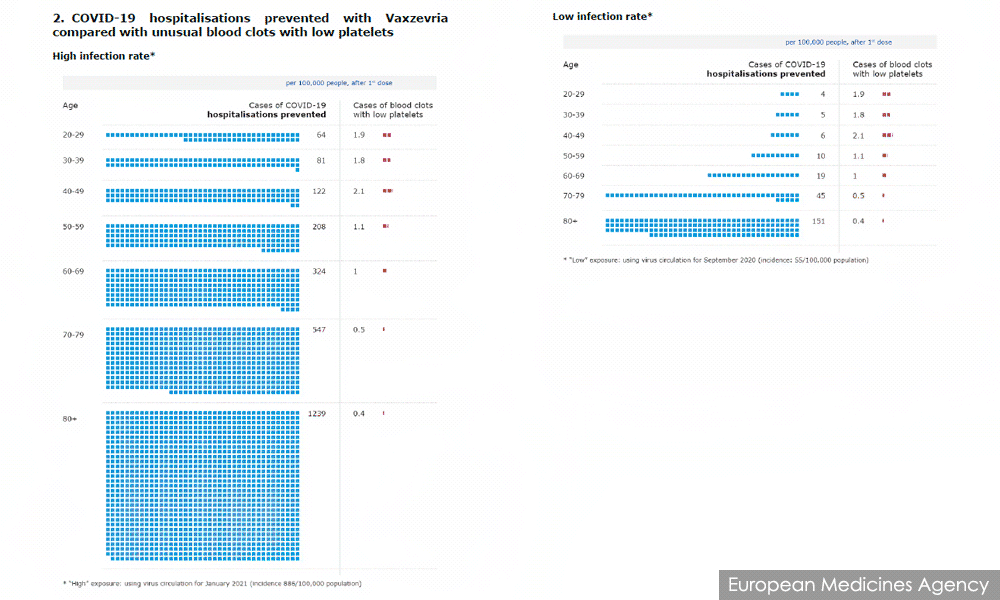
Another issue is the risk of blood clots associated with the AstraZeneca vaccine.
While the risk remains extremely low and the survival rate of these clots has improved since it was first identified, these risks are harder to justify in certain situations.
For example, the benefits of the vaccine are diminished in situations where the prevalence of Covid-19 is low and alternatives to the AstraZeneca vaccine are widely available.
Younger people also see diminishing returns in low-risk situations because they are simultaneously at a lower risk of being hospitalised for Covid-19, while at a higher risk of getting the blood clot.
These considerations of risk-versus-benefit have led some countries that can afford to do so to limit the use of the AstraZeneca vaccine to older age groups, while others continue to recommend it for all adults.
However, discontinuing AstraZeneca vaccinations for younger people has left them in limbo, particularly if they’ve already received the first dose. Part of the motivation for studying heterologous prime boosting is to investigate this issue.
Lastly, knowing that vaccines remain safe and effective when mixed-and-matched doses give governments more flexibility in their vaccine deployments.
If one vaccine becomes unavailable due to supply disruptions, another might be used as a substitute instead of delaying the vaccination programme.
Which countries are already doing this?
According to Reuters, Bahrain and the United Arab Emirates (UAE) are offering vaccines from Pfizer-BioNTech and Sinopharm as third-dose booster shots.
In the UAE capital of Abu Dhabi, the Pfizer-BioNTech vaccine is available to those who completed their Sinopharm vaccination at least six months earlier. A different vaccine can also be used at the recipient’s discretion.
It has also been offering the Sinopharm third-dose boosters after it was found that some recipients did not produce enough antibodies.
Bahrain, meanwhile, is offering the Pfizer-BioNTech or Sinopharm vaccines as booster shots, regardless of what vaccines were initially taken.
In Canada, National Advisory Committee on Immunization (Naci) said on June 1 that people who received the AstraZeneca vaccine as their first dose may receive vaccines from Pfizer-BioNTech or Moderna as their second.
It updated this advice yesterday to say that mRNA vaccines from Pfizer-BioNTech or Moderna are now the preferred vaccines for completing a vaccine series that started with the AstraZeneca vaccine.
“People who received two doses of AstraZeneca/CovidShield vaccine can rest assured that the vaccine provides good protection against infection and very good protection against severe disease and hospitalisation,” it added.
It also said mRNA vaccines are preferred for starting a vaccine series, unless it is inaccessible or contraindicated.
It said it has changed its recommendations in light of the increasing availability of mRNA vaccines in Canada, emerging evidence of improved immune response when the doses are mixed, and the risk of rare blood clots associated with viral vector vaccines.
It cited one of the German studies mentioned above to back its claims of an improved immune response.
“Naci's previous recommendation - that people who wanted earlier vaccination could receive a viral vector vaccine rather than wait for an mRNA vaccine - reflected the limited supply of mRNA vaccines at the time and the imperative of protecting vulnerable populations from serious illness and death from Covid-19,” it said.
South Korea is the latest country to adopt the practice, announcing today that 760,000 people who received their first dose of the AstraZeneca vaccine will be offered the Pfizer-BioNTech vaccine for their second dose.
According to Reuters, this is because the country is facing delays in receiving shipments of the AstraZeneca vaccine from the Covax vaccine-sharing scheme.
This instalment of KiniGuide is compiled by KOH JUN LIN.