Sinovac's Covid-19 vaccine: Old but still gold?
KINIGUIDE | Some view CoronaVac as an inferior product compared to mRNA vaccines, others see it as safer.
KINIGUIDE | Of the three Covid-19 vaccines currently in use in the government’s National Covid-19 Immunisation Programme (NIP), perhaps one of the more divisive ones is Sinovac’s CoronaVac.
On one hand, some view it as an inferior product compared to mRNA vaccines like Pfizer-BioNTech’s Comirnaty due to its poor efficacy in trials, especially when CoronaVac was tested in Brazil.
Meanwhile, proponents view it as a safer vaccine because it was manufactured using the tried-and-true method of inactivating viruses, as opposed to mRNA vaccines (like Comirnaty) and viral vector vaccines (like AstraZeneca-Oxford’s Vaxzevria and CanSino Biologic’s Convidecia) that are relatively new.
The conversation online is further inflamed by the politics surrounding vaccines and their perceived country of origin.
For this instalment of KiniGuide, we cut through the noise to look at the facts and data regarding the vaccine.
Where does CoronaVac fit into the NIP?
Malaysia has thus far made bookings for about 79.5 million vaccine doses, which is enough for 41.5 million people (129.7 percent of the population). The surplus is for dealing with contingencies such as late deliveries and in case some vaccines are rejected by the National Pharmaceutical Regulatory Agency (NPRA).
The figure comes down to 56.8 million doses if vaccines yet to be approved by the NPRA are excluded. This is enough for 28.4 million people (88.8 percent of the population), which should cover all adults in the country.
This includes an order for 12.8 million doses of Comirnaty signed on May 21 to help expedite the vaccination programme.
Of the total orders, CoronaVac accounts for 12 million doses, which is enough for 18.75 percent of the population.
Why is Pharmaniaga involved in this?
Sinovac is a private company based in China, but the deal is facilitated by another agreement between the governments of Malaysia and China that would see Malaysia get priority for vaccines produced in China.
The five-year agreement also includes public and private sector partnerships aimed to help Malaysia develop its own vaccine manufacturing capabilities in the future.
Thus, Sinovac has partnered with the Malaysian government-linked company Pharmaniaga such that the latter would purchase Sinovac’s vaccines in bulk and fill-and-finish it into smaller bottles in its facility in Puchong, Selangor.

A similar partnership has been struck between another China-based company, CanSino Biologics, and local firm Solutions Biologics.
The fill-and-finish process is not a trivial matter. Like any injectable drug, the manufacturing process has to be tightly controlled to prevent contaminants from entering the end-product and ultimately injected into someone’s arm.
Nevertheless, Pharmaniaga has passed 10 weeks of testing and inspections by the NPRA.
Upon the NPRA’s recommendations, the Drug Control Authority first granted conditional approval for CoronaVac and the production facilities in Beijing on March 2, and then Pharmaniaga’s facilities on April 23.
The “conditional approval” means Sinovac and Pharmaniaga must regularly update the NPRA as more data on the vaccine become available over time, so the regulator can ensure the benefits of using the vaccine justifies its potential risks. This is the same for all Covid-19 vaccines being used.
For the NIP, Malaysia uses a mix of CoronaVac vaccines finished at Sinovac’s Beijing facility and those finished at Pharmaniaga’s Puchong facility.
Pharmaniaga will only be supplying the vaccine to other buyers - whether state governments or the private sector - once the federal government’s entire order of 12 million doses have been fulfilled.
The government expects to receive all 12 million doses by the end of July, according to NIP’s coordinating minister Khairy Jamaluddin.
Who is eligible and how is it administered?
According to the patient information leaflet for the vaccine that is available from NPRA’s website, the vaccine can be used by people above 18 years old. It is not currently recommended for people below 18 years old due to limited data on the vaccine's safety and efficacy for this age group.
It is also not recommended for those who are allergic to any of the vaccine’s components or had an allergic reaction to the first dose of CoronaVac or any other vaccine.
Other groups that should not receive this vaccine are those who have severe neurological conditions, uncontrolled severe chronic illnesses and women who are pregnant or breastfeeding.
It should be administered as two 0.5ml doses given two to four weeks apart, although in practice, the dosing interval is only two weeks. This is the shortest of the three vaccines currently in use in the NIP.
The injection is given intramuscularly to the upper arm.

Medical issues aside, the vaccine is not used on haj pilgrims for the time being. The Saudi government has made Covid-19 vaccination mandatory for incoming pilgrims in this year’s haj season, but it does not recognise the Sinovac vaccine.
In response to this, Khairy had said the government is working to ensure the Covid-19 vaccinations in Malaysia are internationally recognised.
In the meantime, prospective haj pilgrims will be offered vaccines made by Pfizer-BioNTech or AstraZeneca instead.
How well does it work?
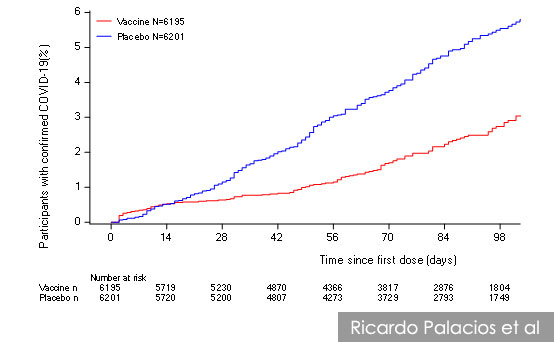
CoronaVac’s performance varied greatly between each clinical trial and even analysis of real-world results.
So far, efficacy estimates are available from three clinical trials in Brazil, Turkey, and Indonesia, according to data compiled by the World Health Organization’s (WHO) Strategic Advisory Group of Experts (Sage) on Immunisation up to April 29.
In Turkey, efficacy was as high as 84 percent against any symptomatic Covid-19 infection, but the figure is lower in Indonesia (65 percent) and among healthcare workers in Brazil (51 percent).
This means that, at least in Brazil, CoronaVac barely meets the WHO’s threshold of what constitutes an acceptable Covid-19 vaccine.
Outside of clinical trials, the vaccine’s performance is similar – 67 percent in one study in Chile and 50 percent in Brazil. This time, however, some Covid-19 variants of concern are in circulation, including the Gamma variant (also known as the P.1 lineage) that is associated with reduced vaccine efficacy.
More importantly, however, the vaccine fully protected against hospitalisation and death caused by Covid-19 across all three clinical trials. It was also 85 percent effective in preventing Covid-19 hospitalisation in Chile.
Recently, on May 12, Indonesian authorities announced another study among healthcare workers that found the vaccine to be 94 percent effective in lowering the risk of symptomatic Covid-19 infections.
Meanwhile, the Uruguay government said CoronaVac reduced deaths by 95 percent, intensive care admissions by 92 percent, and Covid-19 infections by 61 percent.
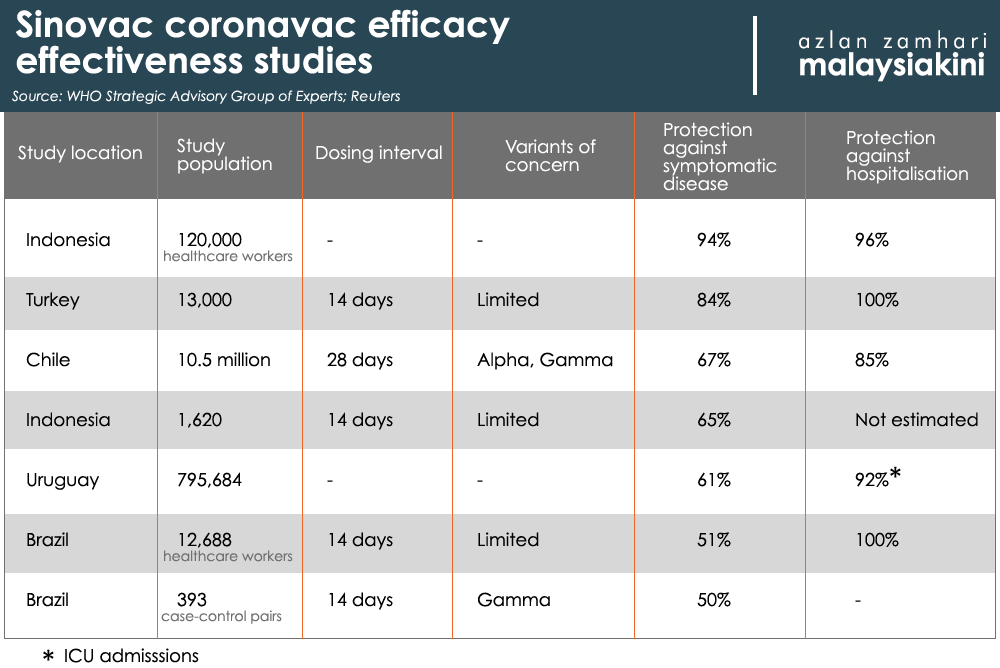
They also reported that Pfizer-BioNTech’s Comirnaty prevented 94 percent of ICU admissions and deaths, and reduced infections by 78 percent. However, the group that received the vaccine was of an older age group than those who got CoronaVac in Uruguay.
Perhaps CoronaVac’s most compelling success story comes from a test in the town of Serrana in Brazil, the results of which were announced through a press conference on May 30.
There, Butantan Institute researchers divided up the town into four areas and fast-tracked their vaccinations to see how well the vaccine performs in the real world.
They succeeded in fully vaccinating about 27,000 people (96 percent of the eligible adults) in just eight weeks, and saw cases start falling by the time they finished administering the second dose to the first group.
When the third group received the second dose, which would mean bringing vaccination rates to about 75 percent of the eligible population, the outbreak was already under control.
The vaccinations were carried out between February and April this year. Eighty percent of all vaccines administered was the CoronaVac vaccine.
“The results were dramatic. Symptomatic cases of Covid-19 have dropped by 80 percent since the start of mass vaccination, related hospitalisations fell 86 percent, and deaths plummeted 95 percent, the research team in charge of the experiment reported during a press conference on May 30.
“Meanwhile, cases have risen out of control in 15 other cities nearby,” Science magazine reported.
The success came despite the Gamma variant being the most common variant in Serrana during the study.
The Butantan Institute is a Brazil state-owned research institute that also produces the CoronaVac in partnership with Sinovac.
Why did the study findings vary so greatly?
WHO’s Sage highlighted several key differences between studies that could influence results.
Most notably, it said the study on Brazilian healthcare workers involved frontliners treating Covid-19 patients, who are also more likely to get tested.

This combination of higher exposure and more frequent testing means trial participants may be more likely to catch Covid-19 than in other trials, and test positive even with very mild symptoms that might have been missed in other trials.
The definition of what counts as a symptomatic Covid-19 infection also varied between trials.
Some quarters believed the circulation of Covid-19 variants of concern in Brazil is also a factor in the study, but Sage said this was unlikely to be the case, at least in the healthcare workers study in Brazil.
“The P.1 (Gamma) variant was not circulating at any of the Brazil trial sites (at the time) and so is not a current hypothesis to explain differences in efficacy,” it said.
In addition, the study in Chile not only has the Alpha (B.1.1.7) and Gamma variants in circulation, but was also performed with a longer dosing interval of four weeks instead of two.
Sage said there is some data suggesting an interval of three weeks or more would give the vaccine a higher efficacy, but more data is needed to see if there is a real difference.
What about the variants of concern?
It is not yet clear how well CoronaVac would perform against the Alpha (B.1.1.7), Beta (B.1.351), and Delta (B.1.617.2) variants of Covid-19, which are circulating in Malaysia.
Of particular concern is the Beta variant that was first detected in South Africa and is the most prevalent of the three variants of concern circulating in Malaysia.
The Beta variant is associated with reduced efficacy of the current crop of Covid-19 vaccines, thanks in part to certain mutations it has in common with the Gamma variant.
What are the risks?
Like all vaccines, CoronaVac has some side effects even though it is based on technology that has been tried and tested, and the risks are deemed to be very low.
These effects will be different for each person and some may not have any side effects at all.
According to the NPRA, some of the more common ones reported in clinical trials include pain and swelling at the injection site, tiredness, diarrhoea, drowsiness and nausea.
These effects should go away in a few days, but if they don’t, you are advised to see a doctor.
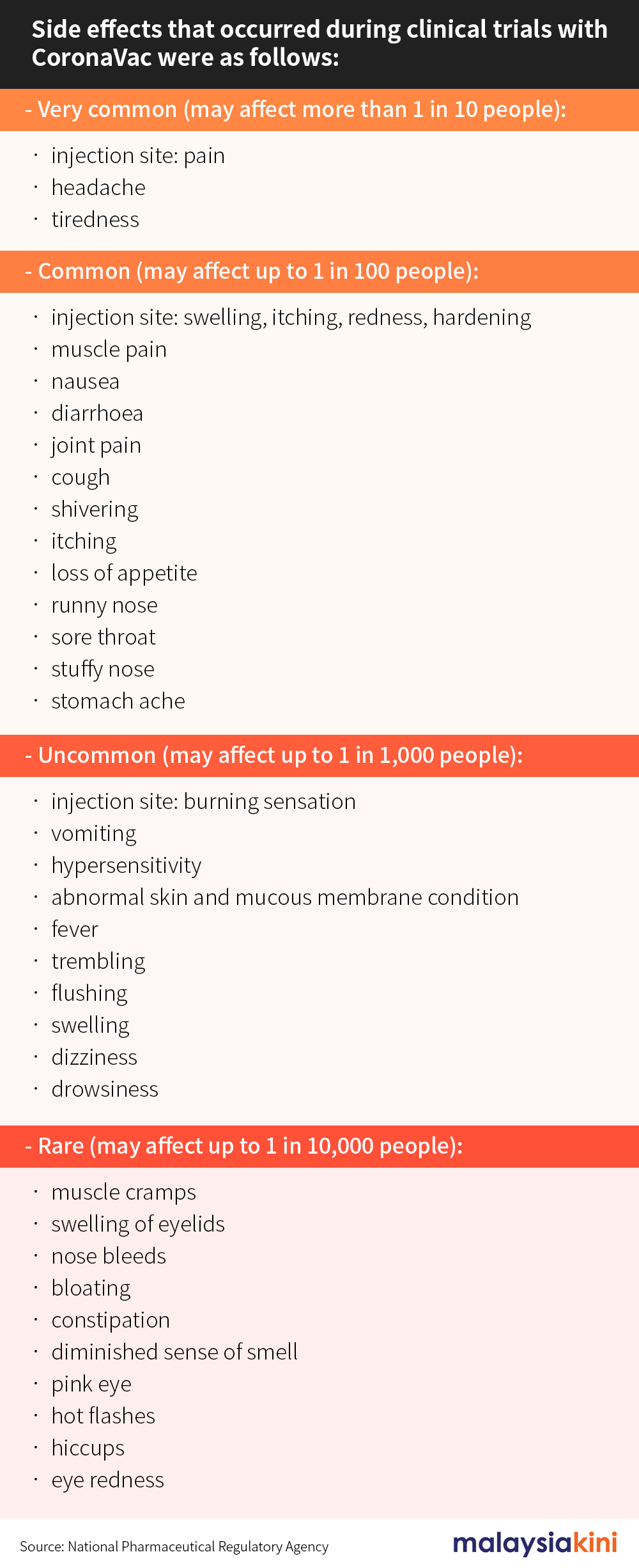
You are also advised to report side effects through MySejahtera or the NPRA’s website, especially if you don’t see it on the list below. This helps authorities monitor the safety of the vaccine as it is being rolled out.
As far as serious adverse events go, none in the clinical trials have been linked to the vaccine and no “safety signals” were identified.
Meanwhile, the WHO’s Sage, which also assessed safety monitoring data following the vaccine’s rollout in China, Brazil, Indonesia and Chile, said no important risks have been identified.
However, it advised increased monitoring for the possibility that the vaccine might heighten the risk of Covid-19 in certain cases.
This is probably due to a slightly increased number of vaccinated people catching Covid-19 and developing symptoms after receiving their first dose and were still waiting for their second dose.
The effect was seen in the clinical trial involving Brazilian healthcare workers, and during the vaccine’s rollout in the country. However, this finding is not yet conclusive.
“Data from other Phase 3 trials in Indonesia and Turkey will be important to give support to or refute this interim finding,” the Sage panel said.
As for the risk of severe allergic reactions (anaphylaxis), no cases were reported among the 8,840 people who received it in various clinical trials across the world.
However, some cases have been reported in the subsequent rollout after the vaccine received approval. The reporting rate is 0.17 reports per million doses in China and 16.9 per million doses in Chile.
For comparison, the reporting rate of anaphylaxis linked to the Pfizer vaccine is 11.1 cases per million. The typical rates for flu vaccines are around 1.4 per million, and the herpes vaccine is around 9.6 per million, according to the US Centers for Disease Control.
Anaphylaxis is a potentially life-threatening condition, but its rapid onset means cases are usually caught during the 15 to 30-minute observation period after vaccination. This allows medical staff to intervene quickly with effective medication.
What is the WHO Sage and why does it get cited in this KiniGuide?
One of the challenges of compiling this KiniGuide is the lack of information available, particularly in the form of peer-reviewed studies from late-stage trials. Instead, most information comes in the form of press releases and announcements with little supporting details.

This changed when Sage held a meeting on April 29 to decide whether or not to recommend that another WHO panel should grant emergency use listing for the Covid-19 vaccines developed by Sinovac and Sinopharm.
Sage is a group of independent experts that advises the WHO on matters relating to vaccines, including those for preventing other diseases. The meeting’s agenda included presentations by Sinovac representatives, and the slides from both Sinovac and Sage members have been made public.
Further, when the WHO ultimately decided to grant emergency use listing for the Sinovac vaccine last week, more information has been published, including Sage’s recommendations, background information and a “scorecard” that Sage used to rate the evidence presented to it.
The documents also include previously unpublished data that are now made public through Sage, with Sinovac's permission, and information gleaned from questioning Sinovac representatives.
In its reports, Sage identified shortcomings in the quality of data in several areas, such as the lack of people over 60 years old participating in the studies and data on severe adverse events.
Nevertheless, it decided: “The data reviewed by WHO support the conclusion that the known benefits of Sinovac-CoronaVac outweigh the risks that are known or considered possible.”
Sage’s assessments and its move to publish detailed information regarding its deliberations have been invaluable in the preparation of this KiniGuide.
RELATED KINIGUIDES:
AstraZeneca round 2: How to sign up and what to know?
How safe is the Pfizer vaccine and how was it done so quickly?
Vaccines vs Variants: What we know so far?
This instalment of KiniGuide is compiled by KOH JUN LIN.